
Adhesive Capsulitis
Adhesive Capsulitis
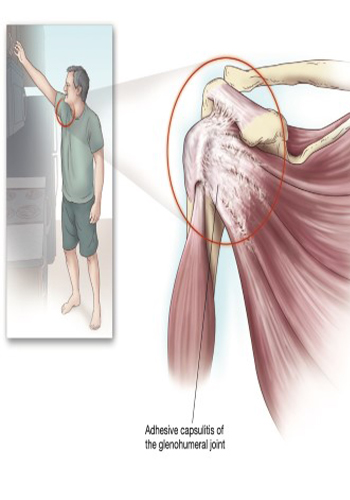
Clinical Syndrome
The shoulder joint is susceptible to the development of various conditions that cause damage or inflammation of the articular cartilage, ligaments, tendons and soft tissues. Although most of these conditions can cause pain and functional disability a positive result is expected when de is properly intervened. However, in some patients, increased pain and inflammation lead to the development of edema and stiffness in the soft tissues and connective tissues of the shoulder, and the movement of the joint it causes the formation of fibrous adhesions, which severely restrict its december. If this condition is not treated, it can result in severe pain and disability. Most of the patients presenting with shoulder pain secondary to adhesive capsulitis, shoulder and he complains of pain localized around the upper arm. Activity exacerbates the pain, rest and heat provide some relief. The pain is continuous and characterized by soreness, whichcan wake you up from sleep. Some patients have joint with its use, they complain of a feeling of tightness or bursting, and on physical examination, crepitation may be present. In addition to pain, patients with adhesive capsulitis note that due to a decrease in the patency of the shoulder movement, the person’s hair they often experience a gradual decrease in their functional abilities due to the fact that it is difficult for them to perform simple daily tasks, such as combing, wearing a bra, or lying on their head. When not used at all, november loss occurs it may come and develop a dull shoulder. Sleep disturbance is quite common in patients with adhesive capsulitis, and sleep can exacerbate the patient’s pain.
Treatment
The initial treatment of pain and loss of function associated with shoulder adhesive capsulitis includes a combination of NSAIDs or COX-2 inhibitors and physical therapy. Local application of hot and cold may also be useful. For patients who do not respond to these methods of treatment, intraarticular injection of local anesthetics and steroids is the next step. Physical methods, including local heat therapy and soft joint range of motion exercises, it should be administered to the patient a few days after the injection due to shoulder pain. Severe exercise should be avoided, as this will increase the patient’s symptoms. Affected due to the underlying reflex sympathetic dystrophy treatment of the limb with stellate ganglion blocks should be started at an early stage of the course of the disease. Shoulder adhesive capsulitis is a common complaint encountered in clinical practice. Rotator cuff tears, including shoulder pain should be differentiated from other causes of shoulder pain. Diseases other than the shoulder area may be responsible for the development of adhesive capsulitis and should be diagnosed and treated if a successful clinical outcome is expected. Arthritis of the shoulder intraarticular injection is extremely effective in the treatment of associated pain. Concomitant Bursitis and tendonitis can contribute to shoulder pain, and october local injections with local anesthetics and methylprednisolone as additional therapy it may require. Simple analgesics and NSAIDs or COX-2 inhibitors can be used simultaneously with this injection technique.